Each Tablet contains: Nifedipine 30 mg.
Pharmacology: Nifedipine is a calcium antagonist of the 1,4-dihydropyridine type. Calcium antagonists reduce the transmembranal influx of calcium ions through the slow calcium channel into the cell. Nifedipine acts particularly on the cells of the myocardium and the smooth muscle cells of the coronary arteries and the peripheral vessels.
In the heart nifedipine dilates the coronary arteries, especially the large conductance vessels, even in the free wall segment of partially stenosed areas. Further, nifedipine reduces the vascular smooth muscle tone in the coronary arteries and prevent vasospasm. The end-result is an increased poststenotic blood flow and an increased oxygen supply. Parallel to this, nifedipine reduces the oxygen requirement by lowering peripheral resistance (afterload). With long-term use nifedipine can also prevent the development of new atherosclerotic lesions in the coronary arteries.
Nifedipine reduces the smooth muscle tone of the arterioles, thus lowering the increased peripheral resistance and consequently the blood pressure.
At the beginning of the nifedipine treatment there may be a transient reflex increase in heart rate and thus in the cardiac output. However, this increase is not enough to compensate for the vasodilation. In addition nifedipine increases sodium and water excretion both in the short-term and long-term use. The blood-pressure-lowering effect of nifedipine is particularly pronounced in hypertensive patients.
Pharmacokinetics: Niferin SR 30mg tablets are formulated to provide nifedipine at an approximately constant rate over 24 hours. Nifedipine is released from the tablet at a zero-order rate by a membrane-controlled, osmotic push-pull process. The delivery rate is independent of gastrointestinal pH or motility. Upon swallowing, the biologically inert components of the tablet remain intact during gastrointestinal transit and are eliminated in the faeces as an insoluble shell.
Absorption: After oral administration nifedipine is almost completely absorbed. The systemic availability of orally administered nifedipine immediate release formulations (Nifedipine capsules) is 45 to 56 % owing to a first pass effect. At steady-state the bioavailability of Nifedipine tablets ranges from 68 to 86% relative to Nifedipine capsules. Administration in the presence of food slightly alters the early rate of absorption, but does not influence the extent of drug availability.
Plasma drug concentrations rise at a controlled rate after Nifedipine dose and reach a plateau at approximately 6 to 12 hours after the first dose. Following multiple days of dosing, relatively constant plasma concentrations at this level are maintained with minimum peak to trough fluctuations over a 24 hours dosing interval (0.9 to 1.2ng/mL).
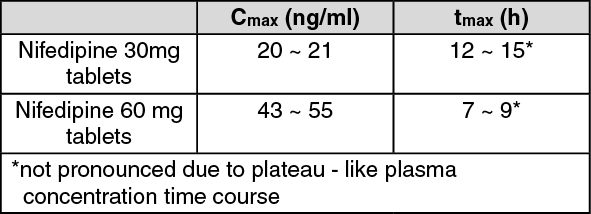
Table: Peak plasma concentrations (C
max) of Nifedipine tablets and the time to reach the peak plasma concentrations (t
max): (See table.)
 Click on icon to see table/diagram/image
Distribution:
Click on icon to see table/diagram/image
Distribution: Nifedipine is about 95 % bound to plasma protein (albumin). The distribution half-life after intravenous administration has been determined to be 5 to 6 minutes.
Biotransformation: After oral administration nifedipine is metabolised in the gut wall and in the liver, primarily by oxidative processes. These metabolites show no pharmacodynamic activity.
Nifedipine is excreted in the form of its metabolites predominantly via the kidneys, and about 5 to 15 % via the bile in the faeces. The unchanged substance is recovered only in traces (below 0.1 %) in the urine.
Elimination: The terminal elimination half-life is 1.7 to 3.4 hours in conventional formulations (Nifedipine capsules). The terminal half-life after Nifedipine Tablets does not represent a meaningful parameter as a plateau- like plasma concentration is maintained during release from the tablets and absorption. After release and absorption of last dose, the plasma concentration finally declines with an elimination half-life as seen in conventional formulations.
In cases of impaired kidney function, no substantial changes have been detected in comparison with healthy volunteers.
In cases of impaired liver function, the total clearance is reduced. A dose reduction may be necessary in severe cases.
Treatment of coronary heart disease: Chronic stable angina pectoris (angina of effort).
Treatment of hypertension.
* It should be used under doctor's prescription.
Dosage (dose and interval): As far as possible the treatment must be tailored to the needs of the individual. Depending on the clinical picture in each case, the basic dose must be introduced gradually. In patients with impaired liver function, careful monitoring and, in severe cases, a dose reduction may be necessary.
Unless otherwise prescribed, the following dosage guidelines are recommended for adults: For coronary heart disease: Chronic stable angina pectoris (angina of effort) 1 or 2 tablets once daily. (1 × 30 mg/day or 2 × 30 mg/day).
For hypertension: 1 or 2 tablets once daily. (1 × 30 mg/day or 2 × 30 mg/day).
In general therapy should be initiated with 30 mg once daily. Depending on the severity of the disease and the patient's response the dose can be increased in stages to 120 mg once daily.
Duration of treatment: The attending doctor will determine the duration of use.
Administration: As a rule the tablets are swallowed whole with a little liquid, independently of meals. The tablets must not be chewed or broken up.
Symptoms: The following symptoms are observed in cases of severe nifedipine intoxication: disturbances of consciousness to the point of coma, a drop in blood pressure, tachycardiac/bradycardiac heart rhythm disturbances, hyperglycaemia, metabolic acidosis, hypoxemia, cardiogenic shock with pulmonary edema.
Management of overdose in man: As far as treatment is concerned, elimination of the active substance and the restoration of stable cardiovascular conditions have priority.
After oral ingestion thorough gastric lavage is indicated, if necessary in combination with irrigation of the small intestine. Particularly in cases of intoxication with slow-release products like Niferin SR 30 mg Tablets elimination must be as complete as possible, including the small intestine, to prevent the otherwise inevitable subsequent absorption of the active substance. Haemodialysis serves no purpose, as nifedipine is not dialyzable, but plasmapheresis is advisable (high plasma protein binding, relatively low volume of distribution).
Bradycardic heart rhythm disturbances may be treated symptomatically with β-sympatiomimetics, and in life-threatening bradycardiac disturbances of heart rhythm temporary pacemaker therapy can be advisable.
Hypotension as a result of cardiogenic shock and arterial vasodilation can be treated with calcium (10 ~ 20 ml of a 10% calcium gluconate solution administered slowly i.v. and repeated if necessary).
As a result, the serum calcium can reach the upper normal range to slightly elevated levels.
If an insufficient increase in blood pressure is achieved with calcium, vasoconstricting sympathomimetics such as dopamine or noradrenaline are additionally administered. The dosage of these drugs is determined solely by the effect obtained.
Additional liquid or volume must be administered with caution because of the danger of overloading the heart.
Niferin SR 30 mg Tablets must not be used in cases of known hypersensitivity to nifedipine.
Niferin SR 30 mg Tablets must not be used in cases of cardiovascular shock.
Niferin SR 30 mg Tablets must not be used in combination with rifampicin because no efficient plasma levels of nifedipine may be obtained due to enzyme induction.
Care must be exercised in patients with very low blood pressure (severe hypotension with systolic pressure less than 90 mm Hg), in cases of manifest heart failure and in case of severe aortic stenosis.
As with other non-deformable material care should be used when administering Niferin SR 30 mg Tablets in patients with pre-existing severe gastrointestinal narrowing because obstructive symptoms may occur. In single cases obstructive symptoms have been described without known history of gastrointestinal disorders.
Niferin SR 30 mg Tablets must not be used in patients with Kock pouch (ileostomy after proctocolectomy).
When dosing barium contrast X-ray Niferin SR 30 mg Tablets may cause false positive effects (e.g. filling defects interpreted as polyp).
Care must be exercised in pregnant women, when administering nifedipine in combination with i.v. magnesium sulfate.
In patients with impaired liver function careful monitoring and, in severe cases, a dose reduction may be necessary.
Fertility: In single cases of in-vitro fertilization calcium antagonists like nifedipine have been associated with reversible biochemical changes in the spermatozoa's head section that may result in impaired sperm function. In those men who are repeatedly unsuccessful in fathering a child by in-vitro fertilization, and where no other explanation can be found, calcium antagonists like nifedipine should be considered as possible causes.
Effect on ability to drive and operate machines: Reactions to the drug, which vary in intensity from individual to individual, can impair the ability to drive or to operate machinery. This applies particularly at the start of the treatment, on changing the medication and in combination with alcohol.
Nifedipine is contraindicated throughout pregnancy, as administration in animals was associated with embryotoxic, fetotoxic and teratogenic effects. All of the doses associated with teratogenic, embryotoxic or fetotoxic effects in animals were maternally toxic and several times the recommended maximum dose for humans. There are no adequate and well-controlled studies in pregnant women.
Nifedipine passes into the breast milk. As there is no experience of possible effects on infants, breastfeeding should first be stopped if nifedipine treatment becomes necessary during the breastfeeding period.
Incidence of frequency ≥1% and <10%: Body as a whole: Asthenia.
Cardiovascular system: Vasodilatation, palpitation.
Digestive system: Constipation.
Metabolic & nutritional disorder: Edema, peripheral edema.
Nervous system: Dizziness, headache.
Incidence of frequency ≥0.1% and <1%: Body as a whole: Malaise, pain.
Cardiovascular system: Angina pectoris (excl, unstable), chest pain, hypotension, postural hypotension, tachycardia, syncope.
Digestive system: Abdominal pain, diarrhea, dry mouth, dyspepsia, flatulence, nausea.
Musculo-skeletal system: Myalgia.
Nervous system: Hypesthesia, insomnia, nervousness, paresthesia, somnolence, vertigo.
Respiratory system: Dyspnea.
Skin and appendages: Maculopapular rash, pruritus, rash, sweating.
Urogenital system: Nocturia, polyuria.
Incidence of frequency ≥0.01% and <0.1%: Body as a whole: Allergic reaction, face edema.
Digestive system: Anorexia, eructation, gastrointestinal disorder, gingivitis, gum hyperplasia, GGT increased, liver function test abnormal, vomiting.
Musculo-skeletal system: Arthralgia.
Nervous system: Tremor.
Respiratory system: Epistaxis.
Skin and appendages: Angioedema, skin disorder, urticaria.
Special senses: Abnormal vision.
Urogenital system: Urinary frequency.
Incidence of frequency <0.01%: Body as a whole: Anaphylactic reaction.
Digestive system: Bezoar, dysphagia, esophagitis, gum disorder, intestinal obstruction, intestinal ulcer, jaundice, SGPT increased.
Hemic and lymphatic system: Leukopenia, purpura.
Metabolic and nutritional disorder: Hyperglycemia, weight loss.
Skin and appendages: Exfoliative dermatitis, gynecomastia, photosensitive dermatitis.
Special senses: Blurred vision.
In dialysis patients with malignant hypertension and hypovolaemia a distinct fall in blood pressure can occur as a result of vasodilation.
Antihypertensive drugs: The blood pressure lowering effect of nifedipine may be potentiated upon co-administration of other antihypertensive drugs.
β-receptor blockers: When nifedipine is administered simultaneously with β-receptor blockers the patient should be carefully monitored, since fairly severe hypotension can occur. Deterioration of heart failure is also known to develop in isolated cases.
Cytochrome P450 3A4: Nifedipine is metabolized via the cytochrome P450 3A4 system, located both in the intestinal mucosa and in the liver. Drugs that are known to either inhibitor to induce this enzyme system may therefore alter the first pass (after oral administration) or the clearance of nifedipine.
Digoxin: The simultaneous administration of nifedipine and digoxin may lead to reduced digoxin clearance and hence an increase in plasma concentrations of digoxin. The patient should therefore be checked for symptoms of digoxin overdosage as a precaution and, if necessary, the glycoside dose should be reduced taking account of the plasma concentration of digoxin.
Quinidine: When nifedipine and quinidine have been administered simultaneously, lowered quinidine or after discontinuation of nifedipine, a distinct increase in plasma concentrations of quinidine have been observed in individual cases. For this reason, when nifedipine is either additionally administered or discontinued, monitoring of the quinidine plasma concentration and, if necessary, adjustment of the quinidine dose are recommended.
Some authors reported increased plasma concentrations of nifedipine upon co-administration of both drugs, while others did not observe an alteration in the pharmacokinetics of nifedipine. Therefore, the blood pressure should be carefully monitored, if quinidine is added to an existing therapy with nifedipine. If necessary, the dose of nifedipine should be decreased.
Cimetidine: Due to its inhibition of cytochrome P450 3A4, cimetidine elevates the plasma concentrations of nifedipine and may potentiate the antihypertensive effect.
Rifampicin: It strongly induces the cytochrome P450 3A4 system. Upon co-administration with rifampicin, the bioavailability of nifedipine is distinctly reduced and thus its efficacy weakened. The use of nifedipine in combination with rifampicin is therefore contraindicated.
Diltiazem: It decreases the clearance of nifedipine. The combination of both drugs should be administered with caution and a reduction of the nifedipine dose may be considered.
Grapefruit juice: It inhibits the cytochrome P450 3A4 system. Administration of nifedipine together with grapefruit juice thus results in elevated plasma concentrations of nifedipine due to an increase of drug bioavailability. As a consequence, the blood pressure lowering effect may be increased.
Theoretical Potential Interactions: Phenytoin: A formal interaction study investigating the potential of a drug interaction between nifedipine and phenytoin has not yet been performed. However, phenytoin is known as a potential inducer of the cytochrome P450 3A4 system. Furthermore, concomitant administration of phenytoin and drugs structurally related to nifedipine clearly reduced their bioavailability. Thus a clinically relevant reduction of the bioavailability of nifedipine cannot be excluded.
Erythromycin: No interaction studies have been carried out between nifedipine and erythromycin. Erythromycin is known to inhibit the cytochrome P450 3A4 mediated metabolism of other drugs. Therefore the potential for an increase of nifedipine plasma concentrations upon co-administration of both drugs cannot be excluded.
Ketoconazole, Itraconazole, Fluconazole: A formal interaction study investigating the potential of a drug interaction between nifedipine and ketoconazole, itraconazole or fluconazole has not yet been performed. Drugs of this class are known to inhibit the cytochrome P450 3A4 system. When administered orally together with nifedipine, a substantial increase in systemic bioavailability of nifedipine due to an increased absorption cannot be excluded. Upon co-administration, the blood pressure should be monitored and, if necessary, a reduction in the nifedipine dose considered.
Tacrolimus: It has been shown to be metabolized via the cytochrome P450 3A4 system. Data recently published indicate that the dose of nifedipine administered simultaneously with tacrolimus may be reduced in individual cases. Upon co-administration of both drugs, the blood pressure should be monitored and, if necessary, a reduction in the nifedipine dose considered.
Interactions Shown Not to Exist: Concomitant administration of nifedipine with Ajmaline, Benazepril, Debrisoquine, Doxazosin, Omeprazole, Orlistat, pantoprazole, Ranitidine has no effect on the pharmacokinetics of either substance.
Aspirin: Concomitant administration of nifedipine and aspirin 100 mg has no effect on the pharmacokinetics of nifedipine. Co-administration of nifedipine does not alter the effect of aspirin 100 mg on the platelet aggregation and bleeding time.
Other Forms of Interactions: Nifedipine may cause falsely increased spectrophotometric values of urinary vanillyl-mandelic acid. However, measure with HPLC is unaffected. Antagonists like nifedipine should be considered as possible causes.
Stored below 30°C. Protect from light and moisture.
C08CA05 - nifedipine ; Belongs to the class of dihydropyridine derivative selective calcium-channel blockers with mainly vascular effects. Used in the treatment of cardiovascular diseases.
Niferin SR tab 30 mg
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
